AnswersPublished8 sources
IVF transfer day ultrasound shows uterine fluid: should you go ahead?
If fluid is confirmed and still present in the endometrial cavity on transfer day, many clinics would postpone or cancel embryo transfer rather than proceed. If the fluid disappears before transfer, frozen embryo transfer data suggest live birth rates may be similar to patients who never had endometrial cavity fluid.
AI Prompt
openai.comCreate a landscape editorial hero image for this Studio Global article: 你是一個ivf expert , 這個女人今天要移植,子宮內膜上超聲波獻示疑似有液體, 還能移植嗎. Article summary: 不建議今天進行胚胎移植。 如果超音波確認子宮內膜腔有液體(endometrial cavity fluid, ECF),尤其是移植當天仍持續存在,多數文獻與常見臨床做法都傾向取消本次移植、密切追蹤或改採後續冷凍胚胎移植(FET)策略。[2][4][5] 這樣做的目的,是先評估可能原因(如輸卵管積水、PCOS、亞臨床子宮感染等)並處理,等下次週期子宮腔乾淨後再移植。[2][3] 若液體在移植前自行消失,後續FET的活產率可與從未出現ECF. Topic tags: deepresearch, general web, workflow, security, privacy. Reference image context from search candidates: Reference image 1: visual subject "cycle is endometrial fluid. This is fluid seen inside the uterine cavity and might come from mucus, blood, inflammatory secretions, or fluid from the fallopian tubes. Doctors usual" source context "Researchers examine how endometrial fluid before transfer affects live birth rates" Reference image 2: visual subject "However, Strandell _et al._ ([20](https://pmc.ncbi.nlm.nih.gov/article
Short answer: if the ultrasound confirms fluid inside the endometrial cavity and it is still there today, transfer is usually not recommended. In IVF, persistent endometrial cavity fluid — often shortened to ECF — around the time of embryo transfer has been linked with poorer implantation or pregnancy outcomes, and a common clinical approach is to monitor closely and cancel the transfer if the fluid remains on transfer day.
This is general medical information, not personal medical advice. Because this decision is time-sensitive, the patient should speak immediately with her fertility specialist or reproductive endocrinologist, who can review the live ultrasound, the amount of fluid, the embryo plan and her history.
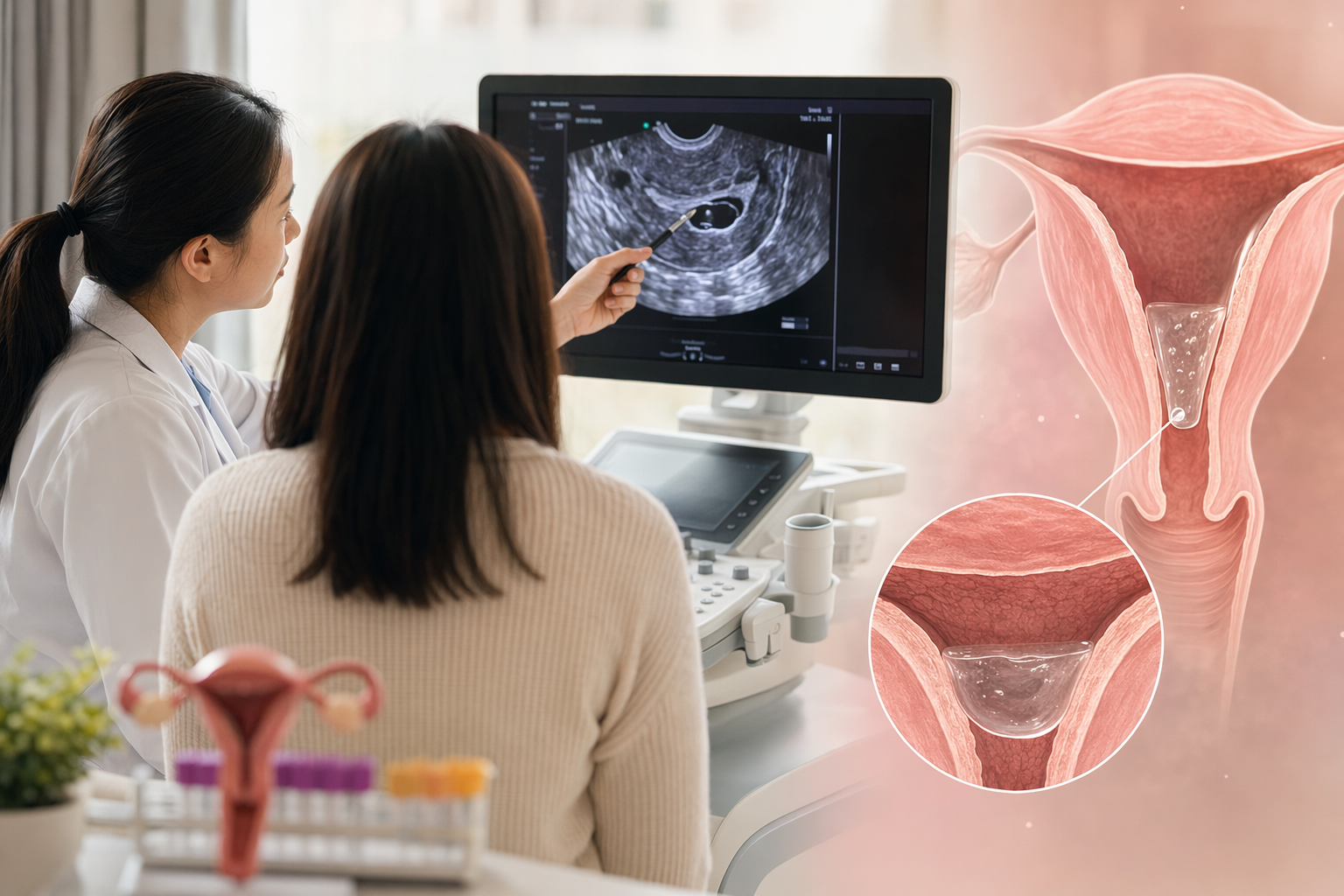
What “fluid in the lining” means
The endometrium is the uterine lining where the embryo is expected to implant. On ultrasound, the uterine cavity is normally more like a closed potential space. A visible pocket or line of fluid between the two sides of the lining is called endometrial cavity fluid.
The key question is not simply “was fluid seen?” but:
- Is it truly inside the endometrial cavity?
- Is it a trace amount or a clear fluid pocket?
- Has it disappeared on repeat scan?
- Is this a fresh IVF transfer or a frozen embryo transfer cycle?
- Is there a possible cause, such as hydrosalpinx, PCOS or subclinical uterine infection?
Why many clinics would cancel if fluid persists today
Several IVF studies and reviews describe fluid within the endometrial cavity before embryo transfer as an unfavourable finding, particularly when it persists close to or on the day of transfer. The concern is straightforward: even a high-quality embryo needs a receptive uterine environment, and persistent fluid may signal that the cavity is not optimal for implantation.
A commonly used management strategy is expectant management with close ultrasound surveillance: keep watching the fluid, proceed only if it resolves, and cancel the embryo transfer if it remains on transfer day.
That is why, if today’s scan truly shows persistent ECF, the safer general answer is: do not proceed unless the treating doctor has a clear reason to judge the risk acceptable.
When transfer may still be considered
There are important exceptions and grey zones.
If the fluid disappears before the actual transfer, evidence from frozen embryo transfer cycles suggests live-birth rates can be similar to those in patients who never had ECF. In other words, a fluid finding earlier in the cycle does not automatically doom the cycle if it resolves before transfer.
There is also some evidence that immediate aspiration of endometrial fluid just before embryo transfer does not necessarily worsen IVF or vitrified-warmed embryo transfer outcomes, and may not reduce implantation in selected cases. But this should not be interpreted as “just remove the fluid and transfer” for everyone. The volume of fluid, the suspected cause and the value of the embryo all matter.
Fresh-cycle evidence is also nuanced: small, transient fluid collections, especially when they disappear and are associated with certain patient factors such as PCOS, may behave differently from persistent or larger collections. Persistent or excessive fluid is the bigger concern.
What the fertility team should confirm right now
Before making a final decision, the clinic should ideally repeat or review the ultrasound and clarify:
- Is there definite fluid or only a suspicious image artefact?
- How much fluid is present? A tiny trace is different from a measurable pocket.
- Is the fluid still there immediately before transfer? Persistence on transfer day is the main red flag.
- What is the endometrial thickness and pattern?
- Is there a history of hydrosalpinx, tubal disease, PCOS or uterine infection? These are recognised associations with ECF.
- Is this a fresh transfer or frozen embryo transfer cycle? The practical options may differ.
Why postponing can protect the chance of pregnancy
Cancelling an embryo transfer can feel devastating, especially when the patient has prepared for this day physically, emotionally and financially. But postponement is often chosen to avoid placing an embryo into a uterine environment that may be less receptive.
If the cycle is postponed, the next step is usually to investigate and address possible causes, then attempt transfer in a later cycle when the uterine cavity is clear. In frozen embryo transfer planning, endometrial preparation may be done through natural, modified natural or hormone-replacement approaches, depending on the patient’s situation and the clinic’s protocol.
The encouraging part: when ECF resolves before transfer, outcomes in frozen embryo transfer cycles may be comparable to those in patients who never had ECF.
Practical questions to ask the doctor today
- “Can we repeat the scan immediately before transfer?”
- “Is the fluid definitely inside the endometrial cavity?”
- “What is the measured size or depth of the fluid pocket?”
- “Do you suspect hydrosalpinx, infection, PCOS-related fluid or another cause?”
- “If we cancel today, what is the plan for the next cycle?”
- “Is aspiration appropriate in this specific case, or would cancellation be safer?”
Bottom line
If endometrial cavity fluid is confirmed and still present on the day of embryo transfer, the evidence and common fertility-clinic practice generally favour postponing or cancelling the transfer rather than proceeding. If the fluid has disappeared before transfer, especially in a frozen embryo transfer cycle, outcomes may be reassuring.
The final call should be made by the treating fertility specialist after real-time ultrasound review and full assessment of the patient’s cycle, history and embryos.
Studio Global AI
Search, cite, and publish your own answer
Use this topic as a starting point for a fresh source-backed answer, then compare citations before you share it.
People also ask
What is the short answer to "IVF transfer day ultrasound shows uterine fluid: should you go ahead?"?
If fluid is confirmed and still present in the endometrial cavity on transfer day, many clinics would postpone or cancel embryo transfer rather than proceed.
What are the key points to validate first?
If fluid is confirmed and still present in the endometrial cavity on transfer day, many clinics would postpone or cancel embryo transfer rather than proceed. If the fluid disappears before transfer, frozen embryo transfer data suggest live birth rates may be similar to patients who never had endometrial cavity fluid.
What should I do next in practice?
The cause matters: endometrial cavity fluid has been associated with hydrosalpinx, PCOS and subclinical uterine infection, among other factors.
Sources
- pmc.ncbi.nlm.nih.govFluid Within the Endometrial Cavity in an IVF Cycle—A ...
- ncbi.nlm.nih.govLive birth rates after resolution of endometrial cavity fluid in frozen embryo transfer cycles
- pmc.ncbi.nlm.nih.govEndometrial cavity fluid is associated with deleterious pregnancy outcomes in patients undergoing in vitro fertilization/intracytoplasmic sperm injection: a retrospective cohort study
- pmc.ncbi.nlm.nih.govThe associated factors to endometrial cavity fluid and the relevant impact ...pmc.ncbi.nlm.nih.gov › articles › PMC2886001
- pmc.ncbi.nlm.nih.govLive birth rates after resolution of endometrial cavity fluid in ...
- pubmed.ncbi.nlm.nih.govEndometrial fluid aspiration immediately prior to embryo ...
- pmc.ncbi.nlm.nih.govEffect of Endometrial Cavity Fluid On Pregnancy Rate of Fresh ... - NIHpmc.ncbi.nlm.nih.gov › articles › PMC5799933
- pmc.ncbi.nlm.nih.govPreparation of the Endometrium for Frozen Embryo Transfer - PMC